|
||||||||||||||||||||||||||||||||||||
| [ Sadržaj
] [ Indeks autora ]
|
||||||||||||||||||||||||||||||||||||
| UDK 616.24-003.4 COBISS.SR-ID 276243212 |
ISSN 0350-2899. - Vol. 44, br. 1 (2019), |
|||||||||||||||||||||||||||||||||||
|
Prikaz slučaja / Case report Large pulmonaly cyst in nonsmoker
- sporadic finding Biljana
Lazović (1), Mihajlo Korać (1), Vuk Aleksić (1), Branko Lukić (1),
Dejan Stevanović (1), Damir Jašarović (1), Rade Milić (2), Vladimir
Žugić (3) |
||||||||||||||||||||||||||||||||||||
|
Sažetak: Cistična bolest pluća (CLD) je grupa oboljenja pluća
koju karakteriše prisustvo multiplih cisti, definisanih kao
translucencije ispunjene vazduhom ili zone niske atenuacije, oivičene
tankim zidom (uglavnom < 4mm). Često se mešaju sa džinovskim bulama koje
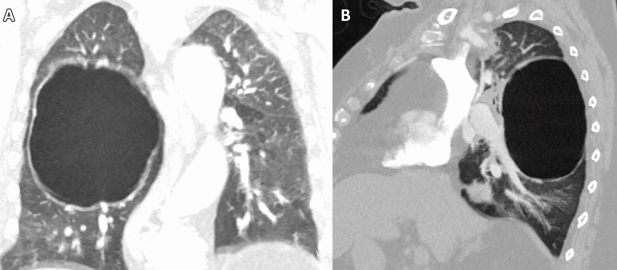
su uobičajene kod pacijenata sa emfizemom. Prikaz slučaja: Žena stara 76
godina sa prethodnom medicinskom istorijom o subokluzivnim smetnjama
primljena je na odeljenje hirurgije. Uzgredno, prilikom preoperativnog
pregleda RTG snimka grudnog koša uočena je džinovska bula u desnom
plućnom krilu. Kompjuterizovana tomografija je potvrdila nalaz, ali zbog
svoje debljine zida promena je svrstana u plućne ciste koje imaju
potpuno drugačiji pristup u lečenju. Zbog toga, pacijentkinja nije
podvrgnuta operaciji i lečena je konzervativno. Zaključak: Glavna
razlika između džinovskih bula i plućnih cisti je debljina zida, ukoliko
je od 1 – 4 mm radi se o plućnoj cisti, za razliku od bule čiji je zid
tanji od 1 mm. Ključne reči: ciste, bule, HOBP, imidžing Summary: Cystic lung disease (CLD) is a group of lung disorders characterized by the presence of multiple cysts, defined as air-filled lucencies or low-attenuating areas, bordered by a thin wall (usually < 4 mm). It is very often mixed with giant bullaes which are common in patients with emphysema. Case report: A 76-year-old woman with a medical history of subocclusive disturbance was admitted to surgery department. Accidentally, during preoperative examination, chest X-ray revealed giant bullae in the right lung. CT scan confirmed it, but due to the wall thickness the changes have been classified into pulmonary cyst which have a completely different approach in treatment. Thus, patient underwent without surgery and was treated conservatively. Conclusion: The main difference between a giant bullae and a pulmonary cyst is in wall thickness, if it measures between 1 and 4 mm it is pulmonary cyst, unlike bullae whose wall is thinner than 1mm. Key words: smokers, cystae, bullae, COPD, imaging |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
Introduction:Cigarette smoking is the major risk factor for the development of
chronic obstructive pulmonary disease (COPD), but not all smokers
develop COPD, and such patients deserve a workup for one of the less
common causes of emphysema. These conditions include A1AT
deficiency, connective issue disease (Cutis laxa, Marfan syndrome,
Ehler-Danlos syndrome), intravenous drug abuse (methylphenidate,
cocaine or talc), HIV infection, hypocomplementemic urticarial
vasculitis syndrome, malnutrition and several rare metabolic
disorders (Salla disease, Menke syndrome).[1] Other differential
diagnoses of bullous emphysema and bullous lung disease include
uncommon causes such as autoimmune diseases (Sjögren disease,
Wegener granulomatosis disease and multisystem autoimmune
dysfunction), bullous sarcoidosis, Birt-Hogg-Dubé syndrome,
neurofibromatosis, placental transmogrification of the lung, Fabry
disease, idiopathic giant bullous emphysema, etc.[2] Almost all
these conditions have systemic manifestation with characteristic
features including early onset, liver dysfunction, vasculitis, skin
and joint manifestations, lymphadenopathy, etc. The evaluation of
bullous emphysema in nonsmokers therefore begins with a detailed
medical history, including age of onset of the disease and a
physical examination, including determination of the presence of
extrapulmonary symptoms or signs and measurement of A1AT level. Discussion:The harmful effects of tobacco smoking, especially with regard to
the aetiology of chronic obstructive pulmonary disease, are well
documented [1, 2]. Large emphysematous bullae
Conclusion:With the increased use of CT, the recognition of CLD has also
increased. HRCT is the most valuable diagnostic modality for an
initial evaluation of CLD as well as bullaes. Along with the
characteristic findings of cysts on CT, the pathologic features,
presence of genetic mutation, and concomitant disease may be helpful
in establishing the differential diagnosis. However, as CLDs are
rare, treatment is currently insufficient. Therefore, enhanced
knowledge of the pathogenesis of CLDs is needed to guide therapeutic
decision-making for each entity. REFERENCES:
|
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Adresa autora / Corresponding
address: Biljana Lazović, University clinical center "Zemun", Vukova 9, Zemun, 11070 Belgrade E-mail: lazovic.biljana@gmail.com |
Rad primljen: 28.2.2019. Elektronska verzija objavljena: 13.5.2019. |
|||||||||||||||||||||||||||||||||||
| [ Sadržaj
] [ Indeks autora ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||