| |
|
|
Introduction
Early Childhood Caries (ECC) is an infectious multifactorial
disease, defined as the presence of one or more surfaces with a
caries lesion (with or without cavitation), missing fillings or
surfaces of teeth (due to caries), on any deciduous tooth among
children up to 71 months [1,2].
Early childhood caries (nursing bottle caries, baby bottle tooth
decay, night bottle mouth, and night bottle caries), as a specific
form of deciduous tooth decay, is characterized by its early onset,
atypical and specific localization, acute flow, rapid complication,
generalization, and often severe consequences. Its incidence leads
to changes in diet due to pain or lack of teeth, the appearance of
dentoalveolar infections, the possibility of damage to the embryos
of permanent teeth, diseases of the digestive tract, frequent
occurrence of respiratory infections, and disorders in the general
physical development of the child [3].
Of great importance is the fact that deciduous dentition caries are
a good indicator of risk for developing caries in permanent
dentition [3,4,5], which is why modern protocols insist on
implementing early prevention in pregnancy and first year of life
[6].
According to relevant research, this is one of the most common
chronic infectious diseases in childhood, which is very difficult to
control due to its multifactorial etiology [7,8].
In the contemporary understanding of the etiology of ECC, the
primary focus is on the conditions that exist in the child’s oral
cavity at the earliest age, which is normally dominated by frequent
lactation, feeding with a bottle, excessive intake of foods rich in
sucrose, as well as the absence of adequate oral hygiene by parents
or caregivers [9].Incorrect eating habits allow the selective
development of aggressive acidogenic forms of streptococcus,
primarily from the Streptococcus Mutans group [10,11].
Obviously, also of particular importance is the amount of cariogenic
bacteria to which the child is exposed in their immediate
environment (family) in the first 18 months, which is designated as
the "gate of infection" [12].
Given this complex etiology, but also the lack of data from the
earliest age, it is considered that any additional research
contributes to solving the problem of caries in the youngest age
[9].
The goal of our research was to determine the frequency of ECC in
children living in the Kosovo Pomoravlje region and identify
possible risk factors for the occurrence of this disease.
Methods
This study was approved by the Ethics Committee of the Faculty of
Medicine University of Pristina, based in Kosovska Mitrovica (No.
09-1559). All clinical trials were performed by two dentists on the
principles of good clinical practice. Kappa statistics were used to
evaluate the reliability of the researchers. Kappa values evaluated
after a review for the intra-consistency of the researchers amounted
to 0.94. The study was carried out in 2017/18, and included 239
children of both sexes, aged 13-71 months, living in rural areas of
the Kosovo Pomoravlje region. Prior to the examination, the parents
were given a written notice detailing the methodology and the
purpose of the research, and requesting written consent for the
participation of children in the study. The parent (guardian) who
gave their consent to the participation of children in the
examination was then interviewed before the child’s dental
examination. Data on social status, attitudes, habits and the
behaviors of the examined children’s parents are recorded in
questionnaires specially designed for this study. Data on caries
prevalence was recorded on a research card which was also designed
for this study according to WHO recommendations and forms an
integral part of the questionnaire. Examinations were conducted
using a dental probe and a mirror under artificial lighting in a
dental chair, in the presence of a parent. Klein-Palmer's DMFT
system was used to indicate caries.
In data evaluation, descriptive and inferential statistical data
methods were used. The descriptive statistical parameters analyzed
the prevalence of caries using the DMFT index (d-decayed, m-missing,
f-filling), the caries tooth index, and the caries average index. As
far as inferential methods, variance analysis, χ2-test (p <0.05) and
logistic regression were used to separate the risk factors from
observed outcome, i.e., caries of early childhood. Each of the
investigated risk factors was analyzed in particular by univariate
logistic regression, and factors that showed statistical
significance were included in the multivariate logistic regression
analysis that separated independent risk factors, that is, the
predictors for the emergence of ECC. In order to analyze the
difference in frequency and between groups, the chi-squared test and
the Fisher test of the exact probability were employed. The
multi-logical regression model included all predictors that had a
statistical significance at the level of 0.05. For the statistical
analysis of the results, the software program SPSS Statistics 22
(SPSS Inc., Chicago, IL, USA) was used.
Results
The total sample was 239 children aged 13-71 months, of which 112
(46.86%) were male and 127 (53.14%) female.
The prevalence of caries in the sample was found to be 56.5%. The
average value of caries index of teeth was 29.1%, and the average
number of affected teeth per respondent was 4.0. Untreated cavities
dominated (94.4%) the DMFT, followed by extracted teeth (3.8%) and a
smaller percentage of sealed teeth (1.8%).
The variables examined - the risk factors for the emergence of ECC
are shown in the tables which follow (Tables 1 and 2), of which the
variables related to the mothers of the examined children are shown
in the first table (Table 1), while those in the second table (Table
2) relate to the child. Each variable is shown in relation to the
incidence of ECC or lack thereof in a particular child.
As statistically significant factors for the emergence of caries of
early childhood, and in relation to socio-demographic
characteristics and habits in the examined mothers, the age of
mothers (Chi-square test =11.162, p =0.004), visits to the dentist
during the pregnancy one or more times (Chi-square test =4.943, p
=0.026) and dental attendance during pregnancy due to teeth problems
(Chi-square test =4.319, p =0.038) (Table 1).
Table 1. Socio-demographic characteristics and habits of the
examined mothers
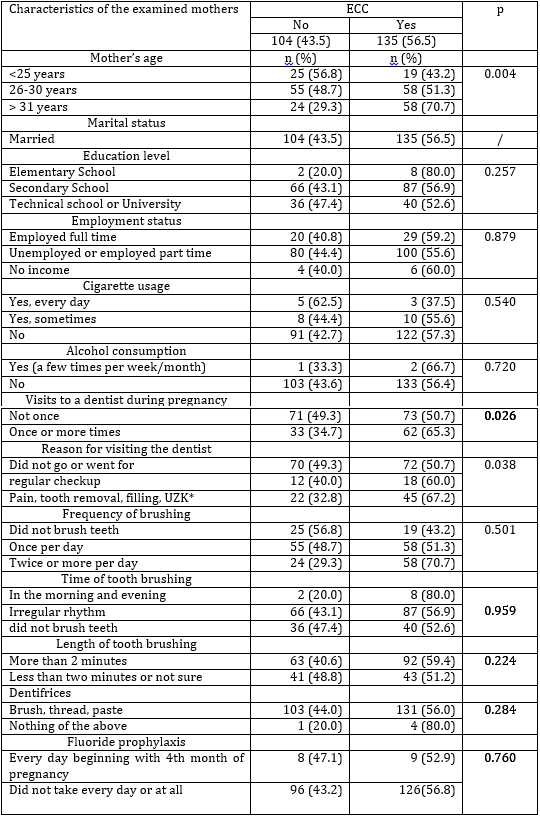
p < 0.05 statistical significance
*UZK - removal of dental calculus
The following variables appeared as statistically significant
factors in the emergence of early childhood caries in relation to
the children’s sex, age and hygienic/dietary habits: the age of
children (Chi-square test = 53.471, p <0.001), birth order
(Chi-square test = 9.917, p = 0.007), use of bottle in feeding
(Chi-square test = 13.394, p = 0.001), and the child’s teeth
brushing habits (Chi-square test = 11.712, p = 0.003) (Table 2).
Table 2. Characteristics of children in relation to sex, age, and
hygienic/dietary habits
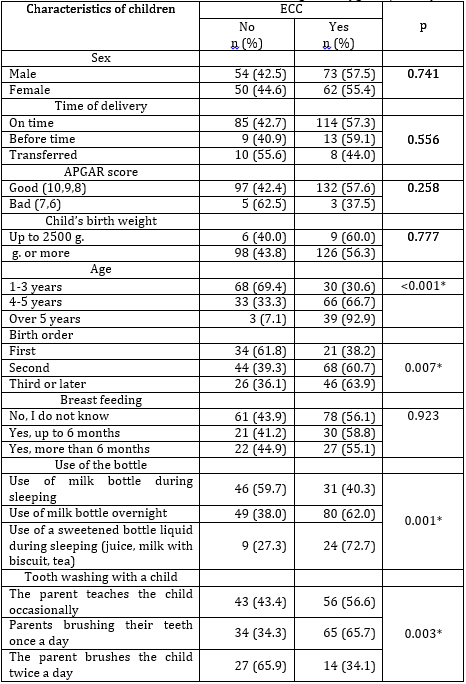
p<0.05 statistical significance
The multiple logistic regression model included all variables that
had a statistically significant association with the onset of early
childhood caries with a significance level of 0.05. The model
contains seven predictors listed in Table 3, which are compared to
239 respondents. The whole model (with all predictors) was
statistically significant (Chi-square test = 75.765, p <0.001). In a
multiple logistic regression model, statistically significant
predictors of early childhood caries are: Bottle feeding [giving a
bottle with milk during the night (B = 0.772; p = 0.028); bottle
feeding with sweetened fluid while putting the child to sleep
(juice, milk with cookies, tea) (B=1.107; p=0.047) compared to the
use of a milk bottle during sleep as a reference category], the
child’s age [age 3-5 (B=1.356; p<0.001), older than 5 (B=3.028;
p<0.001) compared to age 1-3 as a reference category].
Table 3. Multiple logistic regression with the occurrence of early
childhood caries as a dependent variable
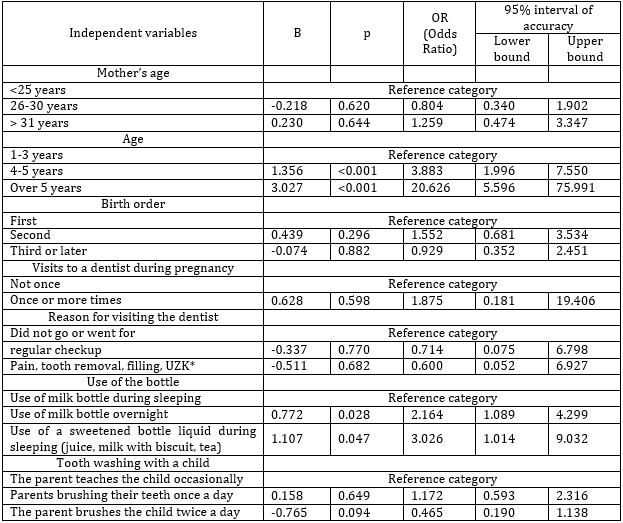
*UZK - removal of dental calculus
The strongest predictor (risk factor) for caries in early childhood
is the child’s age variable, and the age of children older than 5
years, whose risk factor is OR (Odds Ratio) = 20.626. This shows
that children older than 5 years have more than 20 times the risk of
developing caries in early childhood, compared to the controls of
all other factors in the model. Children aged 3-5 years have almost
4 times more risk of developing caries in early childhood.
Also, giving the child a bottle with a sweetened liquid while
putting it to sleep increases the risk of caries by three, that the
child will have caries in early childhood, OR = 3.026, while this
risk is somewhat smaller, OR = 2.164 if the child is given a bottle
of milk overnight.
Discussion
Early Childhood Caries (ECC) is a serious public health problem
in both developed and developing countries around the world due to a
high degree of prevalence. Prevalence is significantly lower in
developed European countries and in the US, if socially vulnerable
groups, immigrants, and individual ethnic communities are excluded
from statistics [13,14,15,16].
Unlike developed countries, the ECC problem in developing countries,
and in particular in our country, it is even more important, because
a large percentage of the infected teeth remain untreated [16, 17,
18].
The prevalence of early childhood caries in this study is 56.5%,
with all subjects aged 13-71 months. This value can be classified as
a high incidence of the disease compared to the prevalence of ECC in
pre-school children in Serbia’s South Backa District [17], in
children up to 24 months in Banja Luka [20], and three-year old’s in
Bulgaria [21].
As is an already recognized fact concerning the occurrence of ECC,
there are large number of factors acting together which result in
ECC, and as far as the possible ECC predictors in our study, with a
significance level of p <0.05, we identify the following seven
statistically significant variable factors: the age of the mother (p
= 0.004), the visits to a dentist during pregnancy (p = 0.026), the
reason for visiting the dentist (p = 0.038), the bottle use in
feeding (p = 0.001), the age of the child (p <0.001), the child’s
birth order (p = 0.007),and the child’s teeth brushing habits (p =
0.003). Our data shows that, the older mothers were, the higher the
incidence of ECC, as confirmed by the fact that 70.7% of children
with mothers over 30 years of age had early childhood caries.
Information in foreign literature speaks of a greater prevalence of
ECC in children whose mothers were younger [22, 23], while in
Serbian authors [24], we find that children of younger mothers had
more severe forms of early childhood caries. The fact that a higher
prevalence of ECC in younger mothers can be explained by lower
education levels and health information available to those mothers.
However, the data which show children having higher instances of ECC
with older mothers can be explained due to a series of
socio-political circumstances, due to which at that time even basic
health education was lacking.
Our study showed that children with more oral health problems (more
frequent visit to the dentist, treatment, or tooth extractions) had
a higher risk for the emergence of early childhood caries. This is
explained by the greater probability of transmission of the
Streptococcus mutans group of bacteria from mother to child, which
is known in literature as "vertical transmission." A number of
studies [25, 26] suggest a direct correlation between the mother's
oral health and the prevalence of ECC in her children.
Eating habits are essential for the development of a cariogenic
dental biofilm and the enhanced acid production. The most important
habits that have a proven connection with the development of ECC are
the improper use of a bottle with cariogenic substances such as
milk, juices, sweetened tea or water, and especially night feeding,
is confirmed in literature [17] and in our research. This finding
point to the need for education of parents about the harmfulness of
such habits, which were significantly related to the emergence of
early childhood caries.
Obradovic`s study in Banja Luka showed that at the age of two,
almost 34% of children have carious lesions [27] and at the age of
three, 48% of children, but also a high prevalence in older ages
with deciduous dentition, such that at the age of six years only 5%
of children without ECC and a caries index average of 8.3 [18].
Our research also shows that as the child grows up, the percentage
of children with ECC increases, and this can be explained by teeth
having been exposed to risk factors for a longer period of time.
As far as the variable of the “Child’s birth order”, our research
showed that the third and every subsequently-born child had
statistically significantly more caries, which is confirmed by
numerous studies around the world and in Serbia [28,29].
An explanation for this claim is the "easier" transmission of
Streptococcus mutans bacteria among children in a collective
environment, as well as between children and other family members,
which is described in literature as "horizontal transmission" [25].
Interestingly, Corrêa-Faria [30] suggests that in families with more
children, the possibility of parental control over oral and hygienic
habits is lessened, and thus the prevalence of ECC in their children
is higher.
That a preschool child is unable to independently and properly
maintain oral hygiene without supervision and help from their
parents is indicated by a higher prevalence of ECC in this age group
in our research, which is also confirmed by other similar studies
[31,32].
Our data indicates, as do other authors [33], that children whose
parents brushed their teeth twice a day had significantly less
caries than children who wash their teeth only once a day or
occasionally.
This necessitates the need for the promotion of oral health as well
as the health education of parents, and therefore of their children.
Considering the fact that Kosovo Pomoravlje is the region with poor
knowledge of the parents about preventive dental treatments [34],
poorer oral health of children is expected [35].The high prevalence
of ECC in the region of Kosovo Pomoravlje indicates that this is a
serious health problem that must be dealt with in a planned,
synchronized and continuous manner through systematic prevention and
timely and adequate treatment of ECC.
Conclusion
Our data shows that a mother’s oral health is an extremely
significant factor in whether or not her children will develop ECC.
Thus, it is necessary to work on providing better health information
and parents education, especially mothers, in how to maintain oral
health, as well as on changing habits, attitudes and behaviors so
they would later lead to the improvement of oral health in their
children. In solving the problem, it is necessary to include all
segments of society and work primarily on the diagnosis and
elimination of risk factors for the development of ECC, as well as
the necessary animation of both the user and providers of dental
health services.
REFERENCES:
- Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG5
Selwitz RH. Diagnosing and reporting early childhood caries for
research purposes. J Public Health Dent. 1999; 59:192-197
- American Academy on Pediatric Dentistry; American Academy of
Pediatrics. Policy on Early Childhood Caries (ECC):
Classifications, Consequences, and Preventive Strategies.
Pediatr Dent. 2008-2009;30:40-43
- Clementino M, Gomes M, Pinto-Sarmento T, Martins C,
Granville-Garcia A, Paiva S. Perceived Impact of Dental Pain on
the Quality of Life of Preschool Children and Their Families.
PLOS ONE. 2015;10(6):e0130602.
- Skeie MS, Raadal M, Strand GV, Espelid I, Therelationship
between caries in the primary at 5 years of age and permanent
dentition at 10 yearsof age- a longitudinal study, Int J
Paediatr Dent 2006; 16:152-60
- Anita Alm. Dental Caries and Caries-RelatedFactors in
Children and Teenagers, University of Gothenburg, 2008, ISSN
0348-6672
- Ng MW, Chase I. Early childhood caries: risk-based disease
prevention and management. Dent Clin North Am. 2013;57:1-16
- Harris R, Nicoll AD, Adair PM, Pine CM. Risk factors for
dental caries in young children: a systematic review of the
literature. Community Dent Health. 2004; 21(1):71-85[PMID:
15072476]
- Leong PM, Gussy MG, Barrow SY, de Silva-Sanigorski A, Waters
E. A systematic review of risk factors during first year of life
for early childhood caries. Int J Paediatr Dent. 2013;
23(4):235-50 [DOI: 10.1111/j.1365-263X.2012.01260.x] [PMID:
22925469]
- Nishimura M, Oda T, Kariya N, Matsumura S, Shimono T. Using
a caries activity test to predict caries risk in early
childhood. J Am Dent Assoc 2008; 139:63–71 PMID: 18167387
- Guido J, Martinez Mier E, Soto A, Eggertsson H, Sanders B,
Jones J et al. Caries prevalence and its association with
brushing habits, water availability, and the intake of sugared
beverages. International Journal of Paediatric Dentistry.
2011;21(6):432-440
- Adair SM. Evidence-based Use of Fluoride in Contemporary
Pediatric Dental Practice. PediatrDent 2006; 28(2):133-42
- Feldens CA, Giugliani ER, Vigo Á, Vítolo MR. Early feeding
practices and severe early childhood caries in four-year-old
children from southern Brazil: a birth cohort study. Caries Res.
2010; 44:445–52. doi: 10.1159/000319898 PMID: 20838043
- Leong PM, Gussy MG, Barrow SUY et al. A systematic reviue
during first year of life for early childchood caries,
International Jurnal of Pediatric dentistry, 2013, 23:235-250
- Dülgergil Ç, Dalli M, Hamidi M, Çolak H. Early childhood
caries update: A review of causes, diagnoses, and treatments.
Journal of Natural Science, Biology and Medicine. 2013;4(1):29
- Kawashita Y, Kitamura M, Saito T. Early Childhood Caries.
International Journal of Dentistry. 2011;2011:1-7
- Day BA et al: Prevalence and Measurement of Dental Caries in
Young Children, Pediatric dentistry, 2015, 37:200-16
- Obradović M, Dolić O, Vojinović J, Sukara S. Association
between feeding habits and severe - early childhood caries in
children up to 24 month old, Serbian Dental Journal,2016, 63(3):
117-124
- Tušek I, Carević M, Tušek J. Influence of social environment
on caries prevalence in early childhood:SrpArhCelokLek.
2011;139(1-2):18-24 (Serbian)
- Obradovic M. Oral health of children up to 6 years of age in
Center for pre-school education in the city of Banja Luka.
Master Thesis. Banja Luka: Faculty of Medicine Banja Luka,
Bosnia and Herzegovina. 2010.
- Obradović M, Dolić O, Vojinović J, Sukara S. Association
between feeding habits and severe - early childhood caries in
children up to 24 month old, Serbian Dental Journal, 2016,
63(3): 117-124
- Markova N. Earlychildhoodcaries:cariesinfantiane.
Dissertation. Sofia: UniversityofSofia; 2003.
- Warren JJ, Blanchette D, Dawson DV, Marshall TA, Phipps KR,
Starr D, Drake DR.Factors associated with dental caries in a
group of American Indian children at age 36 months.Community
Dent Oral Epidemiol. 2016;44(2):154-61
- Niji R, Arita K, Abe Y, Lucas ME, Nishino M, Mitome M.
Maternal age at birth and other risk factors in early childhood
caries.Pediatr Dent.2010 ;32(7):493-8
- Tušek I,Carević M,Tušek J. Impact of social environment and
ethnic affiliation on the development of caries in early
childhood. Acta StomatologicaNaissi.2012;28(1):26-28
- Lynch DJ, Villhauer AL, Warren JJ, Marshall TA, Dawson DV,
Blanchette DR, Phipps KR, Starr DE, Drake DR. Genotypic
characterization of initial acquisition of Streptococcus mutans
in American Indian children. J Oral Microbiol. 2015;7:27182
- Retnakumari N, Cyriac G. Childhood caries as influenced by
maternal and child characteristics in pre-school children of
Kerala:an epidemiological study. Contemp Clin Dent.
2012;3(1):2-8
- Obradović M. The prevalence of early childhood caries and
the effects of dental varnishes on initial caries lesions.
Dissertation. Banja Luka: Faculty of Medicine, 2015
- American Academy of Pediatrics. Oral health risk assessment
timing and establishment of the dental home. Pediatrics
2003;111(5):1113-6
- Tušek I. Impact of social environment and ethnic affiliation
on the development of caries in early childhood. Dissertation.
Belgrade: Faculty of Medicine University of Belgrade; 2009.
(Serbian)
- Corrêa-Faria P et al.Factors associated with the development
of early childhood caries among Brazilian preschoolers. Braz
Oral Res, 2013;27(4):356-62
- Policy on Early Childhood Caries (ECC): Classifications,
Consequences, and Preventive Strategies. Reference manual. 2016;
37(6): 15-16
- Tiberia MJ, Milnes AR, Feigal RJ, Morley KR, Richardson DS,
Croft WG, et al. Risk factors for early childhood caries in
Canadian preschool children seeking care. Pediatr Dent.
2007;29(3):201-8
- Cvetković A, Vulović M, Ivanović M,Correlation between
dental health status and environmental factors: nutrition, oral
hygiene and saliva in childrenda, Serbian Dental
J.2006;53(4):217-228
- Mladenović R, Cvetković A, Martinović B, Milojković Z, Arsić
Z, Đorđević F. Awareness, habits and behavior sassociated with
the oral health of children in elementary schools on Kosovo and
Metohia. Praxis medica 2015;44(2):1-5
- Martinović, B., Cvetković, A., Milojković, Z.,
Stošović-Kalezić, I., Mladenović, R., Stevanović, M. The
incidence of dental caries and gingivitis in school-aged
children. Praxis medica, 2016: 45(2), 33-37.
|
|
|
|