|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
| UDK 616.33-002:616.342 |
ISSN 0350-2899, 35(2010) br.1-2 p 32-36 |
|||||||||||||||||||||||||||||||||||
|
Case review Gastric ulcer in duodenum - or duodenal ulcer on polypoid changed heterotopic gastric mucosa - A case review (Ulkus želuca u duodenumu ili ulkus duodenuma na polipoidno izmenjenoj heterotopičnoj sluznici želuca - Prikaz slučaja) Zoran Joksimović (1), Hakija Bašić (2), Dušan Bastać (3) (1) INTERNISTIČKA ORDINACIJA "JOKSIMOVIĆ" BOR , (2) HAKIJA BAŠIĆ - LABORATORIJA "BIOMARKER" NIŠ, (3) DUŠAN BASTAĆ - INTERNISTIČKA ORDINACIJA "DR.BASTAĆ" ZAJEČAR |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Summary: This work presents a rare case of gastric mucosa heterotopia in duodenal bulb with ulceration. During the upper digestive endoscopy of a sixtyseven-year old female patient, we found a polypoid mass with craterous recesses and necrosis. Histopathological review showed that it was heterotopic gastric mucosa of fundus type with signs of chronic gastritis. The urease test for helicobacter pylori was positive. Control endoscopy after therapy showed a regression of inflammatory and necrotic changes. Repeated histopahological review confirms the microscopic picture of fundus gastric mucosa, but without the elements of inflammation. What is discussed is a need for distinguishing heterotopia from metaplasia and neoplasm, whereby histopathological diagnosis plays the main role. Key words: mucosa heterotopia, ulcer, stomach, duodenum Napomena:
kompletan tekst rada na srpskom jeziku |
||||||||||||||||||||||||||||||||||||
INTRODUCTIONHeterotopia in terms of histology means the appearance of normal tissue on abnormal location. Pathogenesis of heterotypic gastric mucosa is unknown until the end, and by the origin it can be congenital and acquired [1]. Heterotopia of gastric mucosa in duodenum was first described in 1927 [2]. The most common endoscopic form of heterotypic gastric mucosa in duodenum is in a form of spotty changes with superficial erosion and/or ulcerations, or in a form of polypoid formation. Polypoid changes of duodenum on a phon of heterotypic gastric mucosa are rare with prevalence of 0.5-2% [3]. Usually, they do not do not exceed 1.5 cm in diameter. They are revealed accidentally or incidentally, because they are often asymptomatic. Symptoms may be initiated when the obstruction or intussusception appears on them or the peptic ulceration is developed on them [4]. Often heterotypic mucosa is a little different from duodenal mucosa and it is recognized only at histopathological examination [5]. THE AIM OF WORKPresentation of duodenum ulcer on a phon of polypoidic heterotypic gastric mucosa as a rare entity. REVIEW OF THE CASEA 67-years old female patient came to an examination on 1/12/2009
due to pains in epigastrium, heartburn, nausea, emesis and
constipation. Discomforts had lasted for a few months and partially
discount on the H2-receptor blockers. By physical findings, we
concluded a painful sensitivity in epigastrium. Upper digestive
endoscopy showed, in duodenal bulb, directly behind pylorus on the
posterior wall, an irregular polypoide mass, diameter about 12 mm,
which in general was 2-3 mm above the level of mucosa bulbous, light
lobic surface and, in the middle, it had a craterous recess and
field of elliptical necrosis of the largest diameter from 3 to 4 mm.
Mucosa of the rest of duodenum to the Vateri papilla was hyperemic.
Diagnosis: Sessil duodenal polyp with ulcer. |
||||||||||||||||||||||||||||||||||||
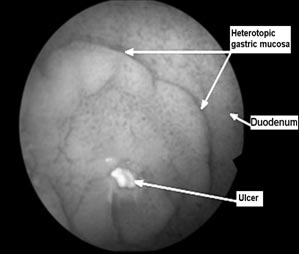 Figure 1 Endoscopic finding |
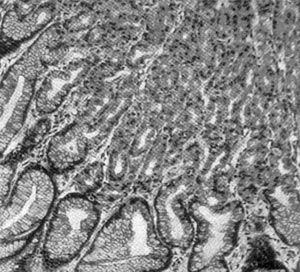 Figure 2 Histopathological finding |
|||||||||||||||||||||||||||||||||||
| The ureasa test for H
pylori from fundous and anthral mucosa was positive. Ultrasound
examination of upper abdomen showed no changes. Total colonoscopy –
diverticulosis of Sigmoid colon was without noticeable changes at
the level of mucosa. The laboratory findings of red and white blood
count and basic biochemical parameters were within reference values. The female patient received the eradication therapy (Omeprazol, Amoxicilin, Metronidazol for a week) and very soon all subjective symptoms disappeared. We continued the therapy with Bismuth and Ranitidine for a month. At the control endoscopy after six weeks (14/1/2010), the ulcerations was repaired “ad integrum” as well as the signs of peptic bulbitis. Polypoid change was unchanged in size and form. The biopsy was repeated and histopathological examination showed the glands of stomach fundous type. Phoveolar regions were with hyperplastic mucin secreting epithelium. The other parts of glands were parietal and general cells. |
||||||||||||||||||||||||||||||||||||
DISCUSSIONHeterotypic gastric mucosa in other parts of the GIT is
macroscopically visible or microscopic re-cognized mainly as
accidental or incidental findings during endoscopy, surgical
intervention or autopsy. The exception is the Mecken's diverticulum
that, in the case of setting up the clinical suspicion, is proved by
radioisotope. Heterotypic gastric mucosa can be found in all parts
of the GIT and outside the digestive tract: mouth, tongue,
oesophagus, larynx, lungs, heart, gall bladder, hepatic ducts,
pancreas, bladder, small intestine, mesentery, colon, rectum, anus
[6, 7, 8]. CONCLUSIONWe presented a rare histopathological phenomenon of polypoid heterotopia of gastric mucosa in duodenum with ulcer. Regarding the endoscopic findings, clinical features, histopathological features of biopted mucosa and the absence of signs of regional enteritis, we concluded that the female patient had a congental gastric heterotopia. Since heterotopia of gastric mucosa had no higher malignant potential as compared to the native mucosa, and the therapy led to the sanation of ulceration and bulbitis, we thought that the patient should not be operated, but only have a regular endoscopic follow. In such cases, histopathological findings are decisive in differential diagnosis of neoplasia. |
||||||||||||||||||||||||||||||||||||
|
|
LITERATURE
|
|||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
|
Corresponding Address: Zoran Joksimović Cara Lazara 12, 19210 Bor e-mail: joksaz@ptt.rs |
Article submitted: 28.01.2010. Article accepted: 11.03.2010. Article Internet issued: 11.11.2010. |
|||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||